1. Lyme Disease (Borrelia species)
From your
Tickborne Diseases 2.0 panel:
- Borrelia burgdorferi (classic Lyme) — IgG positive for multiple antigens:
- VlsE1, C6 peptide, OspB, p41, p34, p45, p66, p83-93, whole-cell lysate (B31 & 297 strains).
- This broad reactivity suggests significant immune recognition — which could be from past or ongoing infection.
- Borrelia bavariensis — IgG + IgM markers present.
- Borrelia mayonii, turicatae, miyamotoi, garinii, afzelii, spielmanii — various IgG positives.
- Many of these are European/relapsing fever strains, so cross-reactivity is possible, but multiple strain hits may point to past tick exposure with more than one Borrelia type.
Takeaway:
You have strong serological evidence of Borrelia exposure. In chronic Lyme, persistent IgG with or without IgM can happen, but serology can’t distinguish active from past infection on its own.
If your ME/CFS symptoms started after a tick bite or flulike illness, Lyme becomes a stronger suspect. PCR or antigen testing on blood/urine/CSF can help confirm ongoing infection.
2. Co-infections (common in chronic Lyme)
You show IgG/IgM positives for:
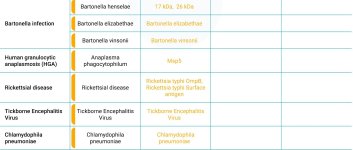
- Bartonella henselae & elizabethae — both associated with neurological symptoms, pain, fatigue, autonomic issues.
- Babesia duncani — malaria-like parasite; causes sweats, air hunger, headaches, POTS-like symptoms.
- Anaplasma phagocytophilum — can cause systemic inflammation and prolonged post-infection fatigue.
- Rickettsia typhi — another intracellular pathogen that can create lingering vascular/neurological effects.
Takeaway:
Co-infections often worsen the severity and chronicity of Lyme symptoms. Your results suggest multiple co-infections, which could explain why ME/CFS-like illness developed or persists.
3. Other infectious load
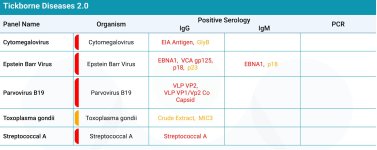
- EBV (Epstein-Barr virus) — IgG positive to multiple antigens (EBNA1, VCA gp125, p18, p23).
This indicates past infection, but in ME/CFS patients, EBV can sometimes reactivate intermittently.
- Cytomegalovirus, Parvovirus B19, Toxoplasma gondii — IgG positives indicate past exposure; some can also cause chronic immune activation if reactivated.
4. Toxin & heavy metal burden
From the
Mycotoxins / Heavy Metals / Environmental Toxins report:
- Aflatoxin G2 — high. Known to impair mitochondrial function & immune regulation.
- Citrinin, Ochratoxin A, Patulin — elevated mycotoxins, all potentially neurotoxic and immune-disruptive.
- Nickel, Barium, Tin — above reference. Metals can impair immune function and increase oxidative stress.
Takeaway:
Chronic Lyme + mycotoxin exposure is a known “synergy” in some ME/CFS cases — both drive inflammation and mitochondrial impairment.
5. ME/CFS relevance
Your lab profile fits a
multi-hit model:
- Primary triggers: Borrelia + multiple tick-borne co-infections.
- Secondary aggravators: Viral reactivations (EBV, possibly CMV), mycotoxins, and heavy metals.
- Result: Chronic immune activation → mitochondrial dysfunction → post-exertional malaise, cognitive issues, orthostatic intolerance, etc.
Next logical steps
If you’re trying to confirm Lyme as
the driver of your ME/CFS:
- Clinical correlation — symptom history, onset timing, Herx reactions to antimicrobials.
- Direct detection tests for Borrelia & co-infections (PCR, FISH, antigen capture).
- Reactivation testing for EBV/CMV (early antigen IgG, PCR viral load).
- Mycotoxin detox assessment — mold exposure evaluation, binders, glutathione status.
- Specialist review — LLMD/ME-CFS specialist to integrate findings and prioritize treatment.